|
Study finds 100% death rate in COVID-19 patients after CPR All 54 COVID-19 patients who underwent cardiopulmonary resuscitation (CPR) in a Michigan hospital died, leading to questions about the risks and benefits of performing a procedure that exposes healthcare personnel to the coronavirus amid limited supplies of personal protective equipment (PPE). The findings, published yesterday in a research letter in JAMA Internal Medicine, found that 52 of 54 patients who experienced cardiac arrest from Mar 15 to Apr 3 (96.3%) had nonshockable rhythms, 44 (81.5%) with pulseless cardiac electrical activity, and 8 (14.8%) with asystole (flatlining). Nonshockable rhythms are those in which the use of defibrillation is highly unlikely to restore a normal heartbeat. Two patients (3.7%) had pulseless ventricular tachycardia (an abnormally fast heart rhythm). CPR achieved a return of spontaneous circulation (ROSC) in 29 patients (53.7%) after a median of 8 minutes. Of the 29 patients, 15 (51.7%) had their code status changed to do not resuscitate, and 14 patients (48.3%) were recoded and underwent additional CPR; all died. Median time from hospital admission to cardiac arrest was 8 days, and median duration of CPR was 10 minutes. At cardiac arrest, 43 patients (79.6%) were receiving mechanical ventilation, 18 (33.3%) were on dialysis, and 25 (46.3%) required vasopressor drugs to treat low blood pressure. Median patient age was 61.5 years, 33 of 54 patients (61.1%) were men, 36 (66.7%) were black, and many had obesity (median body mass index was 33 kg/m2), high blood pressure (42 patients, 77.8%), diabetes (50 [55.6%]), and high cholesterol (27 [50.0%]). Nonshockable rhythms, critical illness: The authors noted that, before the pandemic, 25% of patients who experienced in-hospital cardiac arrest (81% of them with initially nonshockable heart rhythms) survived to hospital release. They attributed the dismal death rate in their study to the high proportion of patients with nonshockable rhythms and those with critical illness requiring mechanical ventilation, dialysis, and vasopressor support—all of which are linked to poor outcomes after in-hospital cardiac arrest. The findings, the researchers said, are similar to those of a Chinese study from early in the pandemic showing a 30-day survival rate of only 2.9% in COVID-19 patients who had in-hospital cardiac arrest. While 94.1% of patients in that study had nonshockable rhythms, only 13% experienced ROSC. The authors called for more studies and the development of guidelines on the risks and benefits of prolonged CPR, an aerosol-generating procedure that can expose healthcare personnel to airborne pathogens such as SARS-CoV-2, the virus that causes COVID-19, in this group of patients. "The transmission of severe acute respiratory syndrome coronavirus 1 [the virus that causes SARS] to health care personnel during CPR has been previously documented," they wrote, referencing a 2004 Canadian study. "Exposure may be further compounded by the limited supply of personal protective equipment nationwide." Critical role of early goals-of-care discussions: In an invited commentary in the same journal, Matthew Modes, MD, MPP, MS; Robert Lee, MD, MS; and J. Randall Curtis, MD, MPH; of the University of Washington in Seattle, pointed out that the lack of effective COVID-19 treatments and delayed initiation of CPR because of the need to first don PPE likely contributed to the 100% death rate. They said that the study findings do not warrant universal do-not-resuscitate orders for coronavirus patients but that they do underscore the importance of discussing goals of care with patients and families early in the course of their illness and again if the patient's clinical status worsens. "Promotion of early goals-of-care discussions should be a priority for patients, families, clinicians, health systems, and policy makers," Modes, Lee, and Curtis said. "Such a shared focus offers substantial opportunity for health system and public health interventions." Because two thirds of the study patients were black, and black patients are less likely than others to have advance care planning documentation and report poor communication with and a lack of trust in healthcare professionals, it is critical for providers to respect individual preferences and foster good communication, the authors of the commentary said."In the context of COVID-19, Black persons and persons of color are more likely to contract COVID-19 or develop serious illness requiring hospitalization; this association is most likely because of disparities," they wrote. "As such, the urgency of eliminating racial disparities in health care has never been clearer." https://www.cidrap.umn.edu/news-perspective/2020/09/study-finds-100-death-rate-covid-19-patients-after-cpr
0 Comments
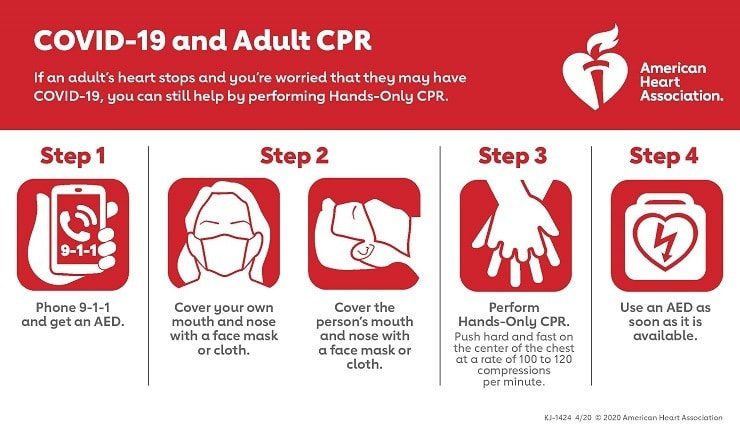 https://www.heart.org/-/media/CPR-Files/Resources/COVID-19-Resources-for-CPR-Training/English/KJ1424_COVID19_and_CPR_Public_200408_ac.pdf
 Amid rushed evacuations, strong winds, and approaching floodwaters of a disaster, chaos often ensues, forcing families to make impossible decisions about the animals that are part of their families. These situations may not always be preventable but having a plan in place can give your pets their best chance of staying safe during and after a hurricane. Keep that plan, and the tools needed to implement it, within an emergency kit tailored specifically to your pet. Here’s the top 10 items recommended for your kit:
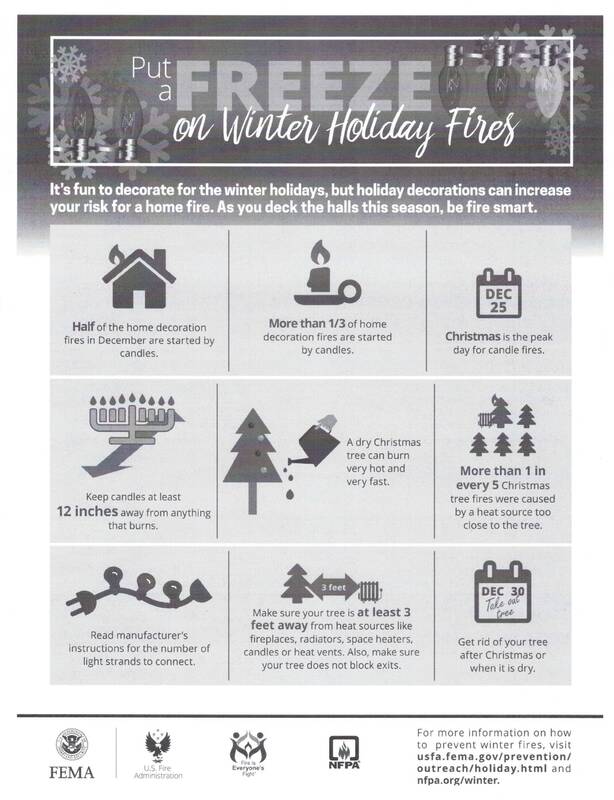    https://www.usfa.fema.gov/prevention/outreach/holiday.html Bystander CPR less likely for black kids in poorest neighborhoods
Journal of the American Heart Association Report Study Highlights: African American kids from the most disadvantaged areas are about half as likely to receive emergency bystander CPR following an out-of-hospital cardiac arrest than white children in disadvantaged or more prosperous neighborhoods. Targeted CPR training for non-white majority, lower education and low-income neighborhoods may increase bystander CPR rates. DALLAS, July 10, 2019 — African American children living in socioeconomically disadvantaged neighborhoods are significantly less likely than their Caucasian counterparts in disadvantaged or wealthier areas to receive CPR from a bystander, according to new research in Journal of the American Heart Association, the Open Access Journal of the American Heart Association/American Stroke Association. Prior studies have examined bystander CPR rates in adults, but this is the first time racial and socioeconomic factors have been analyzed exclusively in children in the United States. An estimated 7,000 children suffer cardiac arrests outside the hospital each year, according to American Heart Association statistics. Investigators at Children’s Hospital of Philadelphia (CHOP) used the Cardiac Arrest Registry to Enhance Survival (CARES) database to examine factors influencing bystander CPR rates for pediatric non-traumatic out of hospital cardiac arrests from 2013-2017. A total of 7,086 cardiac arrests were noted in the CARES catchment area between 2013 and 2017 with 61% occurring in infants, 60% in boys, 31% among white kids, 31% among black kids, 10.5% among Hispanics, 3% other and 24% where ethnicity was unknown. Among the findings: Overall, 3,399 children (48%) received bystander CPR.
“We believe this is the first study to describe the possible role of racial and sociodemographic factors in provision of bystander CPR to pediatric cardiac arrest in the United States,” said lead investigator Maryam Naim, M.D., a pediatric cardiac intensive care physician at CHOP. In 2017, the researchers published initial data from the study, but at that time the reported associations were unclear, noted lead investigator Maryam Naim, M.D. “When analyzing the epidemiology of bystander CPR in children in the United States [in 2017] we found lower bystander CPR rates in black and Hispanic children compared to white children but weren’t sure if this was due entirely to racial disparities or if it was also associated with neighborhood socioeconomic factors like income, employment, and educational status,” said Naim, a pediatric cardiac intensive care physician at CHOP. These results demonstrate a critical need for focused intervention in low-income, non-white, lower education neighborhoods where targeted CPR training might enhance outcomes in children, Naim said. “As most bystander CPR is provided by family members, lower response rates are likely due to a lack of CPR training and recognition of cardiac arrests,” she said, noting that teaching CPR to parents before a newborn is released from the hospital, or during pediatrician visits would be good opportunities for such training. Co-authors are Heather Griffis, Ph.D., Lihai Song, M.S.; Vinay Nadkarni, M.D.; Kimberly Vellano, M.Ph.; Bryan McNally, M.D.; and Rita Burke, Ph.D. Author disclosures are on the manuscript. The Cardiac Clinical Research Core at CHOP funded the study. The CARES registry was funded by the Centers for Disease Control and Prevention until 2012, and today is funded by the American Heart Association, the American Red Cross, Stryker Corporation and Emory University. Statements and conclusions of study authors published in American Heart Association scientific journals are solely those of the study authors and do not necessarily reflect the association’s policy or position. The association makes no representation or guarantee as to their accuracy or reliability. The association receives funding primarily from individuals; foundations and corporations (including pharmaceutical, device manufacturers and other companies) also make donations and fund specific association programs and events. The association has strict policies to prevent these relationships from influencing the science content. Revenues from pharmaceutical and device corporations and health insurance providers are available at https://www.heart.org/en/about-us/aha-financial-information. About the American Heart Association The American Heart Association is a leading force for a world of longer, healthier lives. With nearly a century of lifesaving work, the Dallas-based association is dedicated to ensuring equitable health for all. We are a trustworthy source empowering people to improve their heart health, brain health and well-being. We collaborate with numerous organizations and millions of volunteers to fund innovative research, advocate for stronger public health policies, and share lifesaving resources and information. Connect with us on heart.org, Facebook, Twitter or by calling 1-800-AHA-USA1. For Media Inquiries and AHA/ASA Expert Perspective: 214-706-1173 Bridgette McNeill: 214-706-1135; bridgette.mcneill@heart.org For Public Inquiries: 1-800-AHA-USA1 (242-8721) heart.org and strokeassociation.org CARES Annual Report Shows COVID-19’s Impact On Resuscitation Practices And Outcomes
Without a doubt, the pandemic has posed many challenges for healthcare, including the area of resuscitation. Both healthcare and EMS workers have had to adapt their resuscitation practices. The pandemic’s impact on resuscitation practices in the U.S. is evident in the national dataset collected and presented in the Cardiac Arrest Registry to Enhance Survival (CARES) 2020 Annual Report. CARES helps communities measure standard outcomes for out-of-hospital cardiac arrest, allowing for local quality improvement and benchmarking capability to improve care and survival. AHA is a supporter of CARES. In the U.S., overall survival for out-of-hospital cardiac arrest (OHCA) dropped by 14% in 2020 compared with 2019 (10.5% to 9.0%) and bystander CPR decreased by 2% (41.2% to 40.2%), according to CARES. Below is a summary that captures trends in key OHCA indicators in 2020 that reflect COVID-19’s impact. You can also read this information on page 41.
Time to CPR and Defibrillation Many healthcare professionals and Instructors are familiar with the adage that time is heart. For every minute that passes without CPR and defibrillation, the chances of survival decrease by 7–10%. In March 2020, the average time from cardiac arrest to initial CPR was 6.8 minutes. However, as the pandemic worsened in late summer/early fall, the average time to initial CPR peaked to 8.9 minutes in September, according to CARES. The average time from arrest to defibrillation from January through March 2020 closely followed 2019 levels and began to increase in April 2020. Average time to defibrillation was longer in 2020 compared with 2019 from May to the remainder of the year, per CARES. Patient Outcomes The data in the report shows how the pandemic may have dramatically impacted OHCA survival that may be attributed to factors such as fewer arrests happening in public places, lower rates of bystander CPR, etc. The report notes how 2020 survival rates remained stable from January through March, closely following 2019 rates. However, the report further states the following: overall survival from April 2020 onwards was considerably lower than in 2019, decreasing from a rate of 9.8% in March to a yearly low of 7.1% in December. Notably, the sharpest decrease occurred between March and April, during the onset of the pandemic. Beyond the Pandemic and Knowing Your Community’s Numbers Insights from EMS agencies in three communities and how they adapted their resuscitation practices are featured on page 19 of the report. The lessons learned by these groups – and many other agencies - will likely shape their future resuscitation strategies and practices, which will hopefully result in increased survival rates. To make improvements in OHCA outcomes, it’s crucial that EMS and hospital leaders first know their numbers for key indicators such as bystander interventions and patient outcomes. The data for these indicators submitted to CARES by participating agencies helps EMS and hospital leaders in communities understand how they’re performing compared to others as well as help them determine whether their quality improvement efforts are working. Below are the main questions that CARES helps local EMS administrators and community leaders determine:
About CARES The Cardiac Arrest Registry to Enhance Survival (CARES) is a secure web-based data management system (https://mycares.net) that links the three sources of information that define the continuum of emergency care for out-of-hospital cardiac arrest (OHCA) events: 1) 911 dispatch centers, 2) emergency medical services (EMS) providers, and 3) receiving hospitals, to create a single record for an OHCA event. Registry data collection is critical to improving patient care and survival rates. It allows communities and public health organizations to monitor quality of care, measure and benchmark performance for effective research, and creates a platform for intervention implementation. Communities that participate in CARES can confidentially compare their EMS or hospital system performance using de-identified aggregate statistics at the local, state, or national level to improve their performance in emergency cardiac care. CARES currently includes 29 state-based registries and more than 50 community sites in an additional 15 states, representing a catchment area of approximately 167 million people, nearly 51% of the U.S. population. To read more click here: CARES Annual Report Shows COVID-19’s Impact On Resuscitation Practices And Outcomes https://www.youtube.com/watch?v=lfoTLeFooR4
*check with your employer for OSHA safety regulations. This is an informational video only. Remember Life Jackets:
Half of all boating deaths could be prevented with their use. Learn to Swim: Drowning is the second-leading cause of death in children between ages 1 and 4. Family Safety Plan: It’s important for everyone in the family to be trained in CPR. Secure the Pool: Install fencing with self-closing gates at least 4 feet high to separate the pool from house and yard. Teach Safety: Talk about risky behavior” diving or swimming in unfamiliar water, and alcohol or drug use while in or near water. Clear Out Pool Toys: Make sure children aren’t tempted to play unsupervised. Click on below link to view the AHA water safety infographic: Water Safety Infographic https://www.heart.org/en/healthy-living/healthy-lifestyle/summer-water-safety Summer is synonymous with barbecues, parades and fireworks. The National Safety Council advises everyone to enjoy fireworks at public displays conducted by professionals, and not to use any fireworks at home. They may be legal but they are not safe.
In 2017, eight people died and over 12,000 were injured badly enough to require medical treatment after fireworks-related incidents. Of these, 50% of the injuries were to children and young adults under age 20. Over two-thirds (67%) of injuries took place from June 16 to July 16. And while the majority of these incidents were due to amateurs attempting to use professional-grade, homemade or other illegal fireworks or explosives, an estimated 1,200 injuries were from less powerful devices like small firecrackers and sparklers. Additionally, fireworks start an average of 18,500 fires each year, including 1,300 structure fires, 300 vehicle fires and nearly 17,000 other fires. If consumer fireworks are legal to buy where you live and you choose to use them, be sure to follow the following safety tips:
Sparklers Are Dangerous: Every year, young children can be found along parade routes and at festivals with sparklers in hand, but sparklers are a lot more dangerous than most people think. Sparklers burn at about 2,000 degrees – hot enough to melt some metals. Sparklers can quickly ignite clothing, and children have received severe burns from dropping sparklers on their feet. According to the National Fire Protection Association, sparklers alone account for more than 25% of emergency room visits for fireworks injuries. For children under 5 years of age, sparklers accounted for nearly half of the total estimated injuries. Consider using safer alternatives, such as glow sticks, confetti poppers or colored streamers. https://www.nsc.org/home-safety/tools-resources/seasonal-safety/summer/fireworks Transportation Safety: Whether children walk, ride their bicycle or take the bus to school, it is extremely important that they take proper safety precautions. Here are some tips to make sure your child safely travels to school:
Walkers »Review your family's walking safety rules and practice walking to school with your child.
Backpacks »Choose a backpack for your child carefully; it should have ergonomically designed features to enhance safety and comfort.
https://www.nsc.org/home-safety/seasonal-safety/back-to-school |